 Mindful Clover
Mindful Clover
May 2, 2025
Reclaiming Complexity: New Perspectives on Counseling and Cognition
Introduction
Throughout my training as a graduate student, I found my theoretical home in Carl Rogers’ approach to counseling. His emphasis on empathy, authenticity, and unconditional positive regard didn’t just seem like a good technique—it felt like a worldview, a systematic way of relating to clients on their own terms. Person-centered counseling insists that people matter more than protocols, that interpersonal healing emerges through presence rather than procedure. Strangely, even though Rogers is foundational in counseling education, his approach often feels radical—even subversive―when measured against the clinical norms which dominate the modern practice of clinicians.
Today, mental health professionals work under a system that privileges manualized interventions, randomized control trials, and treatment fidelity. “Evidence-based practice” has become a rallying cry, but the kind of evidence we’ve come to value tends to be narrow, medicalized, and reductionistic.1 These systemic pressures don’t just shape research—they impact how therapy is practiced, reimbursed, and understood by the agencies that pay therapists for their services. A 2023 investigation by ProPublica and NPR found that low reimbursement rates, excessive documentation demands, and opaque insurance policies are pushing many therapists out of network entirely, highlighting just how deeply bureaucratic and economic structures now dictate the shape of mental health care.2
This isn’t to say that therapists want to practice in this way; most will admit they are eclectic and integrative in their approach. Yet the pressure remains, subtly distorting both public and professional understandings of counseling by shifting focus away from its core healing processes. Indeed, this approach risks missing something essential: that the heart of healing lies not in techniques alone, but in the relationship, the context, and the meaning-making that unfold in the therapy room.
This post brings together two critical challenges to that reductionistic ethos. The first comes from within psychotherapy research itself: the common factors movement, which suggests that the elements shared across therapeutic modalities—not their unique methods—are what most reliably produce change. The second comes from the sciences of mind: the growing turn toward embodied cognition, which undermines the assumption that the mind is simply a brain processing information, divorced from body and world.
While I speak more from my clinical experience and research knowledge regarding counseling, I am much more of an enthusiastic spectator of the cognitive sciences. Yet I see how critiques of research in psychotherapy and cognition point toward a shared, crucial insight: What heals, what changes us, and what constitutes knowledge itself is deeply embedded in context, relationship, and embodied experience. What excites me about common factors and embodied cognition is that they aren’t simply reiterating cliches, some off-handed appeals to “holistic approaches” in order to detach from rigorous empirical study. Rather, they ask us to provide deeper, more complex understandings of the mechanisms at play in human healing and growth.
My hope is to show how these insights are not only intellectually compelling, but urgently needed—especially for counselors trying to make sense of our place in an increasingly bureaucratized and medicalized mental health system. And across my practice and research, I have begun to wholeheartedly believe in the following: A counselor’s best tool for becoming more effective is rooted in a project of self-growth toward authentic, genuine engagement with their clients and the world. This post sketches the framework that is leading me toward such a conclusion.
From Competition to Connection: Rethinking a Century of Evidence in Psychotherapy
Socially speaking, the turn from the 19th to 20th century was an interesting time for the professions, including both medicine and talk therapy: Western culture became increasingly captured by a scientific understanding of the world, so being perceived as “scientific” was crucial to garnering resources for your occupation.3
In the attempt to legitimate the talking cure, the earliest pioneers of psychotherapy used many forms of evidence to prove their point. The most famous examples come from the case studies that Freud judiciously used to prove his psychoanalytic theory of the unconscious.4 However, as the century progressed, psychotherapy research increasingly focused on creating experimental conditions that could fit into the rigorous standards seen in the sister field of medicine, especially the “gold standard” of the Randomized Control Trial. Further, psychotherapy is not truly one thing, and much intellectual effort was spent in proving my (CBT, etc.) therapy is better than your (Freudian, etc.) therapy.
Accordingly, across the 1900s the fields of psychotherapy and counseling became increasingly focused on manualizing therapy (to fit the standards of experimental science) and on proving the superiority of individual theoretical approaches (to garner social credibility and funding). This pursuit of scientific legitimacy encouraged competition over cooperation, fragmenting the field into camps and doctrines. Yet as research matured, cracks began to appear in this model. If rigorous trials were meant to crown a single “best” therapy, why did so many different approaches seem to produce similar results? And why did client outcomes often hinge more on the therapist-client relationship than the specific techniques used?
These questions led some researchers to shift focus—not toward inventing new therapies, but toward identifying what all successful therapies share. This line of inquiry, most systematically presented by Bruce Wampold and Zac Imel in The Great Psychotherapy Debate, challenges the assumption that psychotherapy research should slavishly follow medical models. Instead, it asks a different, more profound question: What if it’s not the manualized intervention that heals, but the common factors that emerge across all effective therapies?
This line of questioning takes specific issue with the use of medically-derived methods to “prove” that one manualized therapy or modality is better than another. The result of this competitive approach has been to crown some therapies as “more evidence-based” than others (cue the scary CBT noises). Yet this emphasis has detracted from investigating an arguably more productive research program: What factors underlie all comprehensive therapeutic approaches, regardless of theoretical allegiance? In response to these concerns, researchers began to look beyond individual therapies and toward the elements that are common across all effective forms of psychotherapy.5
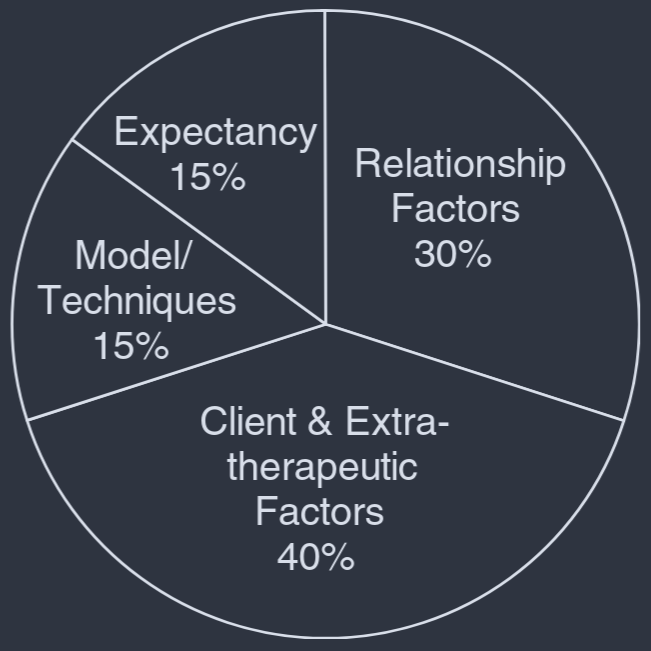
This shift gave rise to what is now known as the common factors theory. It urges researchers to question the traditional philosophical assumptions underlying psychotherapy research and asks practitioners to refocus on what actually drives therapeutic success. According to this perspective, the key ingredients of effective therapy include the therapeutic alliance, the characteristics and extratherapeutic variables of the client, and the characteristics of the therapist6—not the specific techniques or manuals employed.
from Thomas (2016) citing Miller et al. (1997)
“Comprehensive therapeutic approaches” almost sounds circular, but studies have found that it’s near impossible to create a true “sham” condition for randomized-control trials of therapy.7 In other words, in creating a sham condition for counseling, it is no longer counseling. This is because there are core conditions that must be met for a client to think that the therapy is actually therapy. Bruce Wampold highlights this in the following:
“There are a number of trials that compare a coherent, cogent, structured treatment to what’s often called “supportive therapy,” where the patient just sits with an empathic therapist, but there’s no treatment plan, there’s no explanation to the patient about what they’re going to do in therapy to help them get better… [They] are a lot more effective than doing nothing, but they’re not as effective for targeted outcomes as those that have a coherent explanation and treatment plan. As long as what they’re doing is believable, accepted, is given by a therapist who’s skilled and believes in the treatment as well, the treatment tends to go well.” - link
So, rather than investigating “what therapies work, for what type of client, with what type of illness,” we would instead focus on “what are the factors that promote positive change in the context of a comprehensive therapeutic program.” Moving toward these factors resists chopping therapy up into manualized elements and instead demands attention to more subjective phenomena, like the charisma of the therapist and the client’s lived experience of the relationship.
But this shift raises an important challenge: How do you rigorously study something as fluid, dynamic, and context-dependent as human connection? The traditional experimental methods, borrowed from medicine, struggle to capture these relational and experiential elements without flattening them into discrete, decontextualized variables. Instead, the common factors approach broadens the researchers perspective. While it must include the processes and procedures of the specific therapeutic program, it also includes those human, relational dynamics in the room.
This tension—the difficulty of studying lived experience through methods designed for isolated mechanisms—is not unique to psychotherapy. It reflects a deeper philosophical challenge that has surfaced across the sciences of the mind. Cognitive science, too, has been undergoing a quiet revolution: moving away from the view of the mind as a brain-bound information processor, and toward models that emphasize embodiment, embeddedness, and enaction. Just as psychotherapy researchers began to question whether healing could be reduced to isolated techniques, cognitive scientists began to wonder: Can experience itself be captured by a purely neurological framework?
Beyond the Brain: The Embodied Nature of Cognition (and Therapeutic Change)
We often speak as if our minds are just machines housed in our skulls. “I can’t get it to stick in my brain,” we say. Or, “My brain isn’t wired for this,” “That’s just how my brain works,” or even “My brain is fried.” These everyday phrases reveal a deeper cultural metaphor: the idea that we are our brains, and that the complexities of thought, emotion, and experience can be reduced to neural activity. But what if this metaphor, useful as it may be, also limits our understanding of ourselves?
This reductionistic view—one that equates the mind with brain processes alone—has deeply influenced how Western science studies the mind. Yet it leaves little room for the lived texture of experience, or the way our bodies, environments, and relationships shape how we think and feel. In drawing heavily from computer innovations in the 20th century, this model conceives of cognition in terms of information processing, while subjective experience and bodily engagement with the world are seen as secondary or irrelevant. This model inherits a long philosophical legacy: the subject-object split, rooted in Cartesian dualism, which imagines the mind as separate from the body and world.
In response to this brain-focused, computational model of mind, alternative frameworks like embodied and enactive cognition have emerged, emphasizing that thinking is not something the brain does in isolation, but something we do as living, situated beings. The Embodied Mind is a landmark text in this movement, arguing that cognition cannot be separated from the bodily, social, and historical contexts that give rise to it.
This perspective also introduces a powerful tension: any scientific account of cognition is itself a product of the cognitive system it seeks to describe. We cannot study the mind from a clean, external vantage point, because our very act of studying is entangled with the structures and assumptions of our own embodiment. As the authors write:
“The basic assumption, then, is that to every form of behavior and experience we can ascribe specific brain structures… And, conversely, changes in brain structure manifest themselves in behavioral and experiential alterations… Yet upon reflection we cannot avoid as a matter of consistency the logical implication that by this same view any such scientific description…must itself be a product of the structure of our own cognitive system… [T]he act of reflection that tells us this does not come from nowhere; we find ourselves performing that act of reflection out of a given background… But then yet again, our very postulation of such a background is something that we are doing: we are here, living embodied beings, sitting and thinking of this entire scheme, including what we call a background.” (pp. 10-12)
Even our most “objective” descriptions of cognition, then, are entangled within the very system they seek to explain. We cannot step outside of our embodied, contextualized minds to deliver an objective view from nowhere; our observations, methods, and assumptions are all shaped by the biological, experiential, and historical structures we aim to study.
Importantly and essentially, this does not mean that all views are equally valid, as the more extreme forms of socially-constructed nihilism might suggest. It simply means that we must grapple seriously with how our embeddedness in various systems shapes what we can know—and how we know it.
Yet reflection does not liberate us from this embededness; it deepens it. The “background” against which we reflect is not a neutral backdrop—it is itself an active construction of our living, situated minds. As The Embodied Mind suggests, true understanding requires grappling with this recursive, lived nature of cognition, rather than trying to purge it from the science altogether.
This circularity may seem like an abstract problem confined to philosophy or cognitive science, but it has real and urgent implications for how we study psychotherapy. As an example, the recent technological revolution of neurological imaging has found its way into psychotherapy research and practice. Specifically, the allure of “neuro” images―like the fMRI’s depiction of blood flow in the brain―has become a highly-prized piece of evidence in proving “how and why therapy really works.”8 Check out my other post, The Talking Cure of Floating Brains, for a related discussion on my skepticism of this project.
When we imagine that we can isolate and measure “pure” interventions as if from a detached, external vantage point, we risk severing therapy from the human experiences that make it meaningful and effective in the first place. If cognition itself cannot be cleanly separated from the context, embodiment, and lived experience of the thinker, then how much more so is this true for therapy, which is fundamentally about the meeting of subjective worlds?
Conclusion
I see this post as an exercise in sketching some limits of thought, both professional and philosophical, that intrigue me. As a clinician who asks my clients to investigate the way they understand their self & world, I find myself drawn to the same process: What do I take to be true about myself as a counselor, about the profession and practice of counseling, about the way we “prove” that talking with another person “works?”
When and why do we decide to “collapse” one level of explanation into another? In psychotherapy research, the tendency is to reduce the outcomes to the specific intervention used; in cognitive science, that tendency is toward reducing everything to the brain; when these worlds meet, the brain becomes the preeminent evidence for proving therapy’s “real” efficacy. These reductions forget, neglect, and discard the experiences of the humans in the room. However, in reflecting on and integrating our experience into research, I believe we broaden the capacities of our sciences (as in embodied cognition) and our ability to be more effective as practitioners (as in the contextual model). In cognitive science, it means recognizing that the act of studying mind is itself a cognitive, embodied act, situated within a context we cannot escape. In psychotherapy, this means honoring the relational, contextual, and experiential foundations of healing rather than reducing change to isolated techniques or repeated images of the brain.
Footnotes
For a good argument that contests the phrase “evidence based therapy,” see Jonathan Shedler’s Where is the Evidence for Evidence-Based Therapy? (YouTube)↩︎
Why I Left the Network investigates the experiences of over 500 therapists, psychologists, and psychiatrists across the country (link).↩︎
The scare quotes are to emphasize that, while scientific pursuits are among the most rigorous ways humans know the world, being perceived as “scientific” is a social act of assigning value and resources to a person, profession, or institution. That leaves it wide open to the age-old problems of bias, persuasion and personality, bad intentions, and the like.↩︎
For an intriguing read regarding the evolution of Freud’s case studies, see Carl E. Pletsch’s 1982 article, “Freud’s Case Studies and the Locus of Psychoanalytic Knowledge” (pdf link).↩︎
While this line of research is relatively new, proponents of the common factors routinely point to Saul Rosenzweig’s work in the 1930’s as a precursor to this line of questioning.↩︎
See Thomas (2006), “The Contributing Factors of Change in a Therapeutic Process,” for an overview of these factors (publisher link; pdf link).↩︎
“Bruce Wampold on What Actually Makes Us Good Therapists” (Psychotherapy.net article).↩︎
I am about to embark on a journey into Neuro: The New Brain Sciences and the Management of the Mind by Nikolas Rose and Abid-Rached. I imagine it will provide a more systematic analysis of the allure of the “neuro” than I’ve discussed here.↩︎
Previous post The Chaos Machine is required reading The Chaos Machine by Max Fisher is a journalistic tour de force, comprehensive in its coverage of the perils of social media. And there are many.